The emergency department is hard to schedule for the same reason it is hard to work in: there is almost no margin for error.
A weak inpatient schedule can limp along for a while. A weak ED schedule announces itself fast.
The ED Cannot Hide Its Problems
Demand changes quickly. Handoffs happen on a fixed clock. The unit cannot close. If a physician calls out, the problem is not theoretical. It is immediate.
That alone makes ED scheduling different from most hospital scheduling.
The Schedule Is Carrying More Than Coverage
An ED schedule is not just deciding how many people are present. It is also carrying fatigue, handoff quality, supervision, skill mix, and the ability to absorb a bad hour without the whole department tightening up.
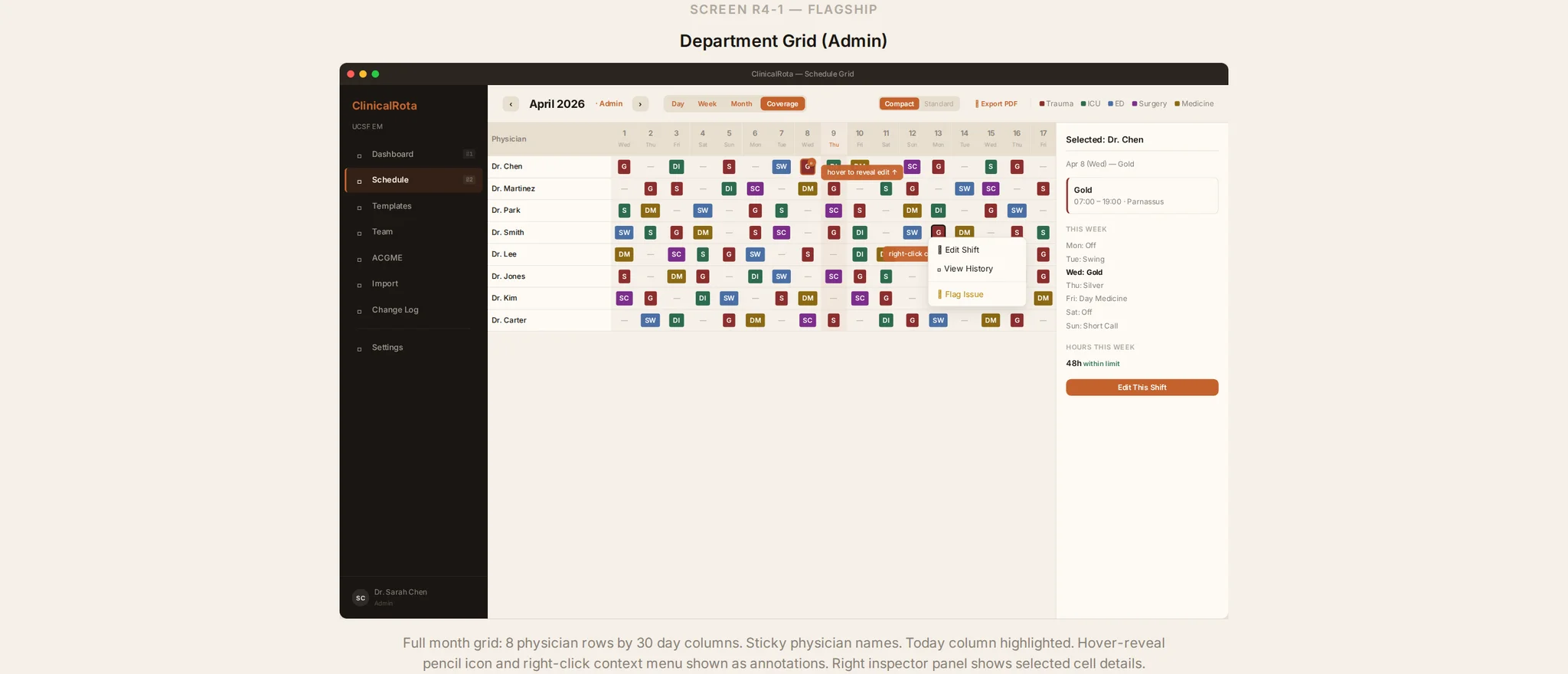
This is why a monthly grid is not enough. The interesting part is often the layer underneath it. Who is on now? Who is already carrying the hard run of shifts? Which nights are thin? Which replacement options are real and which are only nominal?
Change Handling Matters More Than Perfect Planning
A lot of scheduling software is built around publication. The ED cares just as much about recovery.
What happens when the attending is sick? What happens when the department is suddenly busier than usual? What happens when a handoff is going to be rough because the outgoing physician has spent the last two hours in a resuscitation?
The product has to help with those moments or it is solving the wrong problem.
What Better Software Would Actually Do
It would make the weak points visible early.
It would make handoff shape easier to inspect.
It would make backup logic clearer than a phone tree.
And it would let the department see the real schedule, not just the version that looked acceptable at the time it was published.
If ED scheduling in your department keeps failing at the moment reality diverges from the plan, see the sneak peek. We will walk through the current direction, learn where the current workflow breaks first, and decide what the first version should do.